
A $50 Billion Program to Transform Rural Health. Here’s Where It’s Needed Most.

Key Takeaways
- The funding is real – but so is the tension.
The One Big Beautiful Bill Act created a $50 billion Rural Health Transformation Program, distributing $10 billion annually from 2026 through 2030. The same legislation cut federal Medicaid spending by an estimated $911 billion over the next decade, the largest reduction in the program’s history. The RHTP was designed in part to offset those losses, but for rural providers already operating on razor-thin margins, the math is unforgiving. - Wisconsin’s behavioral health crisis is hiding in plain sight.
Farmers, fishers, and forestry workers experience suicide rates 180% above the national average. Binge drinking rates across rural Wisconsin are among the highest in the country, and the treatment infrastructure to respond is concentrated almost entirely in Milwaukee, Madison, and Green Bay. - Georgia’s maternal health crisis is a geographic emergency.
82 of the state’s rural counties have no OB-GYN, and 53 have no hospital at all. The communities with no obstetric capacity are the same ones scoring highest on the Maternal Vulnerability Index, the places where women are most at risk and least able to travel for care elsewhere. - Arkansas is caught in a compounding trap.
The state has the third-highest heart disease mortality rate in the nation, and nearly its entire rural geography simultaneously carries elevated hypertension and coronary heart disease prevalence. The communities bearing that burden are also the most Medicaid-dependent, making them the most exposed to the coverage cuts embedded in the same bill funding the RHTP. - Delaware’s shortage is structural, not incidental.
The state ranks last in the nation for meeting primary care needs, and Sussex County tells the whole story: rural-designated, low health worker concentration, and low bachelor’s degree attainment all converge in the same geography. You cannot recruit your way out of a pipeline problem. Delaware is betting on building one from scratch.
On July 4, 2025, President Trump signed the One Big Beautiful Bill Act into law, and buried inside its nearly 900 pages was something rural health advocates had been fighting for: a $50 billion Rural Health Transformation Program. Administered by CMS, the program distributes $10 billion per year from 2026 through 2030 to states with approved rural health transformation plans. By December 29, all 50 states had submitted applications and received awards averaging around $200 million each for the first year.
The money is real, and it is moving, but context matters. The same legislation that created the RHTP reduced federal Medicaid spending by an estimated $911 billion over the next decade, the largest cut to the program in its history. The RHTP was designed in part to offset those losses for rural providers, who are disproportionately Medicaid-dependent and already operating on razor-thin margins. The average rural hospital operating margin was just 3.1% in 2023, with 44% already in the red.
That tension makes targeting everything. States cannot spread $200 million evenly across hundreds of rural counties and expect meaningful change. They need to know where disease burden is highest, where providers are scarcest, where coverage losses will hit hardest, and where dollars will actually move the needle. That is a geographic data problem, and it is one PolicyMap is built to answer. State plans submitted to CMS coalesced around four themes: workforce development, chronic disease management, behavioral health, and maternal health. Below, we walk through each one.
Behavioral Health: Wisconsin and the Rural Mental Health Crisis
Wisconsin’s RHTP application opens with a striking statistic: workers in farming, fishing, and forestry occupations experience suicide rates 180% above the national average. The state has more dairy farms than any other in the country, and its rural agricultural workforce is bearing an outsized share of a crisis that does not show up in most urban-focused mental health datasets.
Wisconsin’s response centers on a Farmer Wellness Program, a 24-hour helpline, free counseling vouchers redeemable in person or via telehealth, and monthly online support groups. It is a community-based mental health infrastructure designed specifically for a population that is geographically dispersed, culturally resistant to traditional clinical settings, and chronically underserved by the existing system.
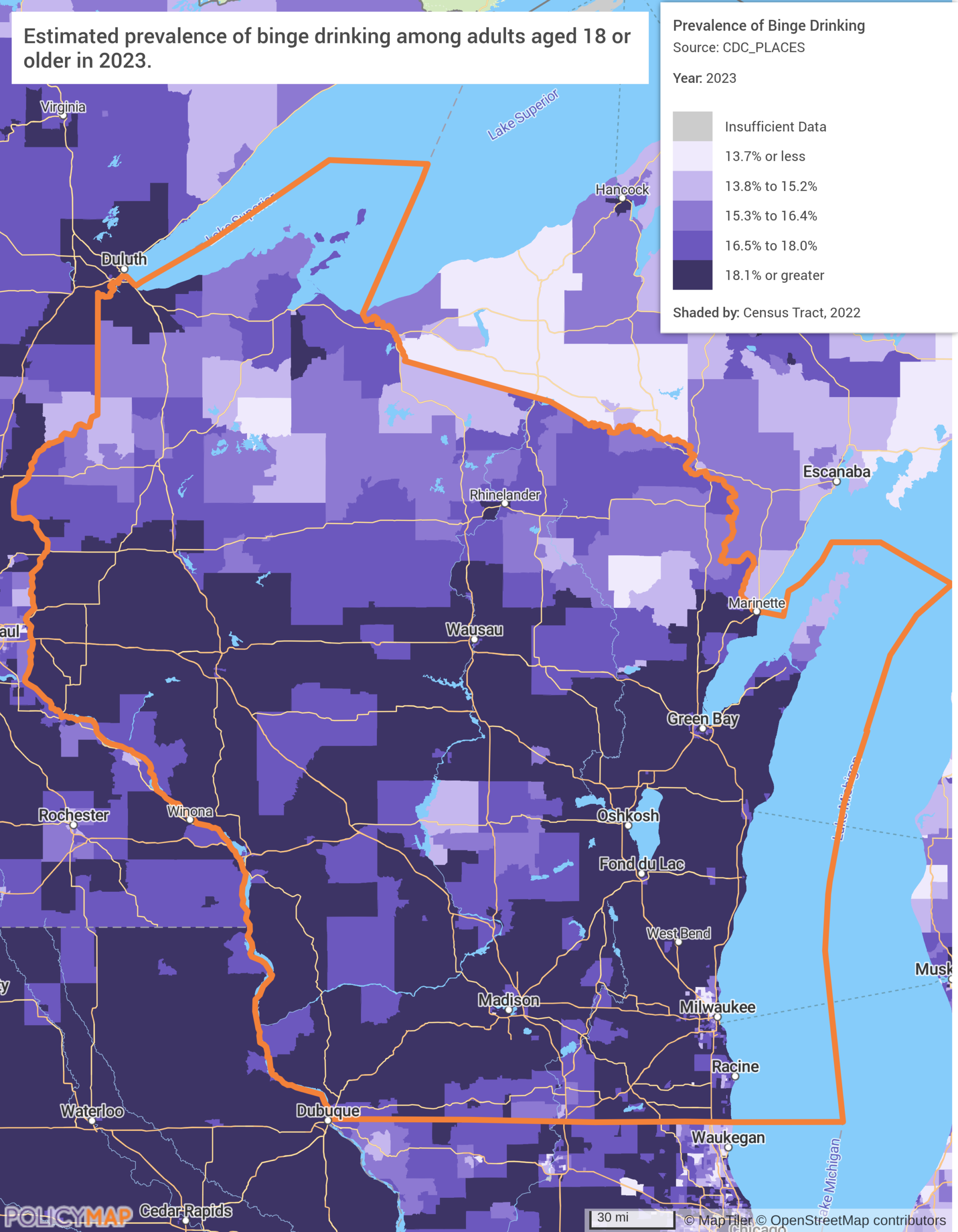
The first map shows binge drinking prevalence across Wisconsin census tracts. Nearly the entire state falls in the darkest categories (noticeably higher than neighboring Minnesota and Michigan), and the rural regions outside of the state’s major cities, where agricultural communities are most concentrated, show the heaviest rates. This is the behavioral side of the crisis.
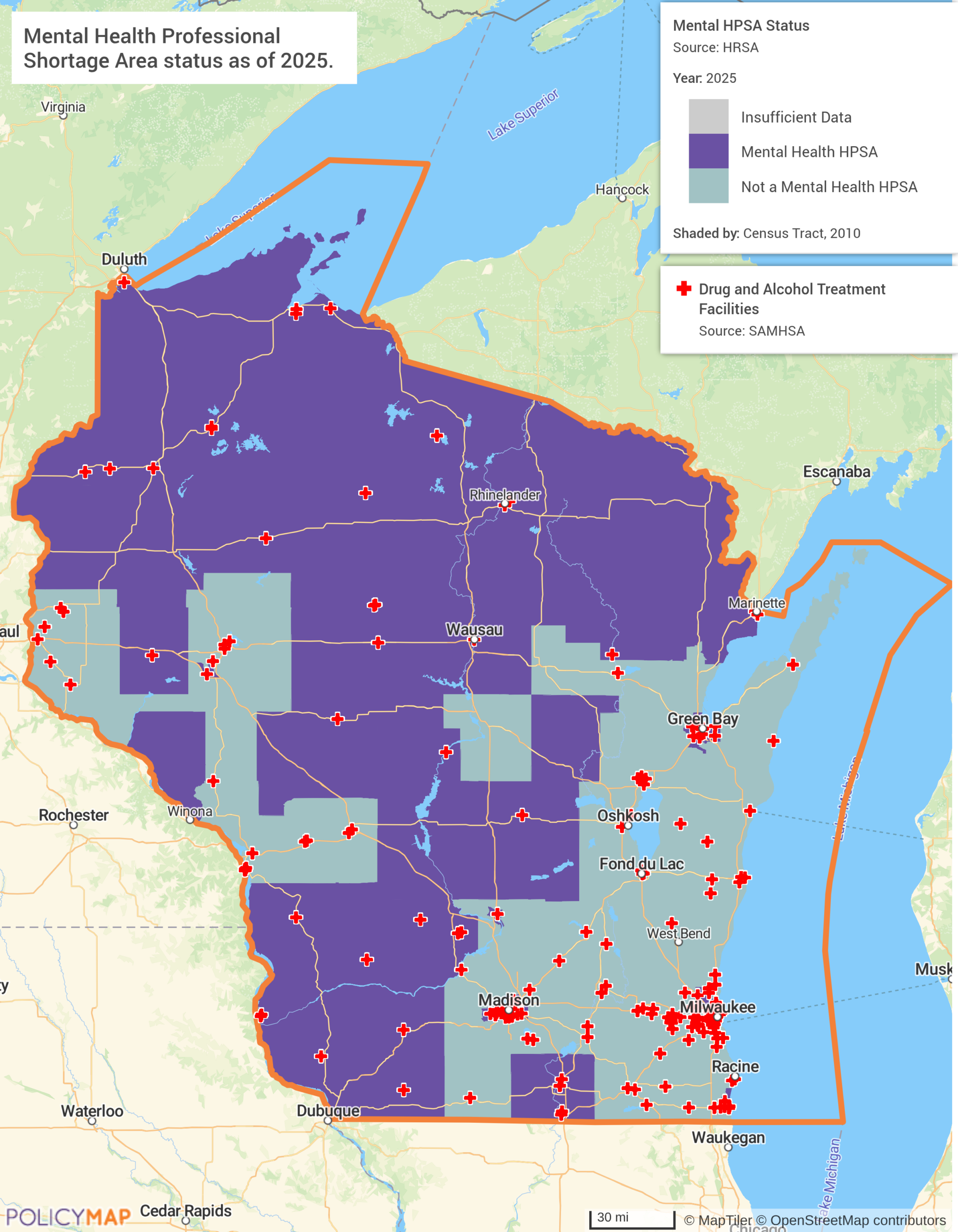
The second map shows where the system exists to respond to it, and where it does not. Mental health HPSA designations cover the majority of rural Wisconsin, and drug and alcohol treatment facilities cluster almost entirely in Milwaukee, Madison, and Green Bay. The vast rural north and west, where drinking rates are darkest on Map 1, has almost no treatment infrastructure at all. The problem is everywhere. The help is not.
Wisconsin is not an outlier. North Carolina is deploying mobile opioid treatment program units and expanding Certified Community Behavioral Health Clinics across rural regions. Connecticut explicitly called out rural emergency departments becoming “de facto mental health systems” and is responding by standing up 23-hour crisis stabilization centers linked to rural hospitals. Washington identified substance use disorder as the leading rural health challenge in the state and is building technology-enabled care models to reach dispersed populations.
Maternal Health: Georgia and the Obstetric Desert Crisis
Of all the data points in all 50 state RHTP applications, Georgia’s stands out: 82 of the state’s rural counties have no OB-GYN, and 53 have no hospital at all. In more than half of Georgia’s rural counties, a woman experiencing a pregnancy complication has no obstetric care available locally. The state’s response, placing obstetric carts stocked with hemorrhage management supplies, neonatal resuscitation equipment, and preeclampsia treatment in non-delivering emergency departments, is less a transformation strategy than a triage measure for a system already in crisis.
Georgia is also creating patient safety bundles across all 66 of its birthing hospitals, with an emphasis on the 15 that are rural. And it is working to address the underlying access gap through hub-and-spoke models, telehealth obstetric infrastructure, and workforce investments targeted at communities where no OB-GYN has practiced in years.
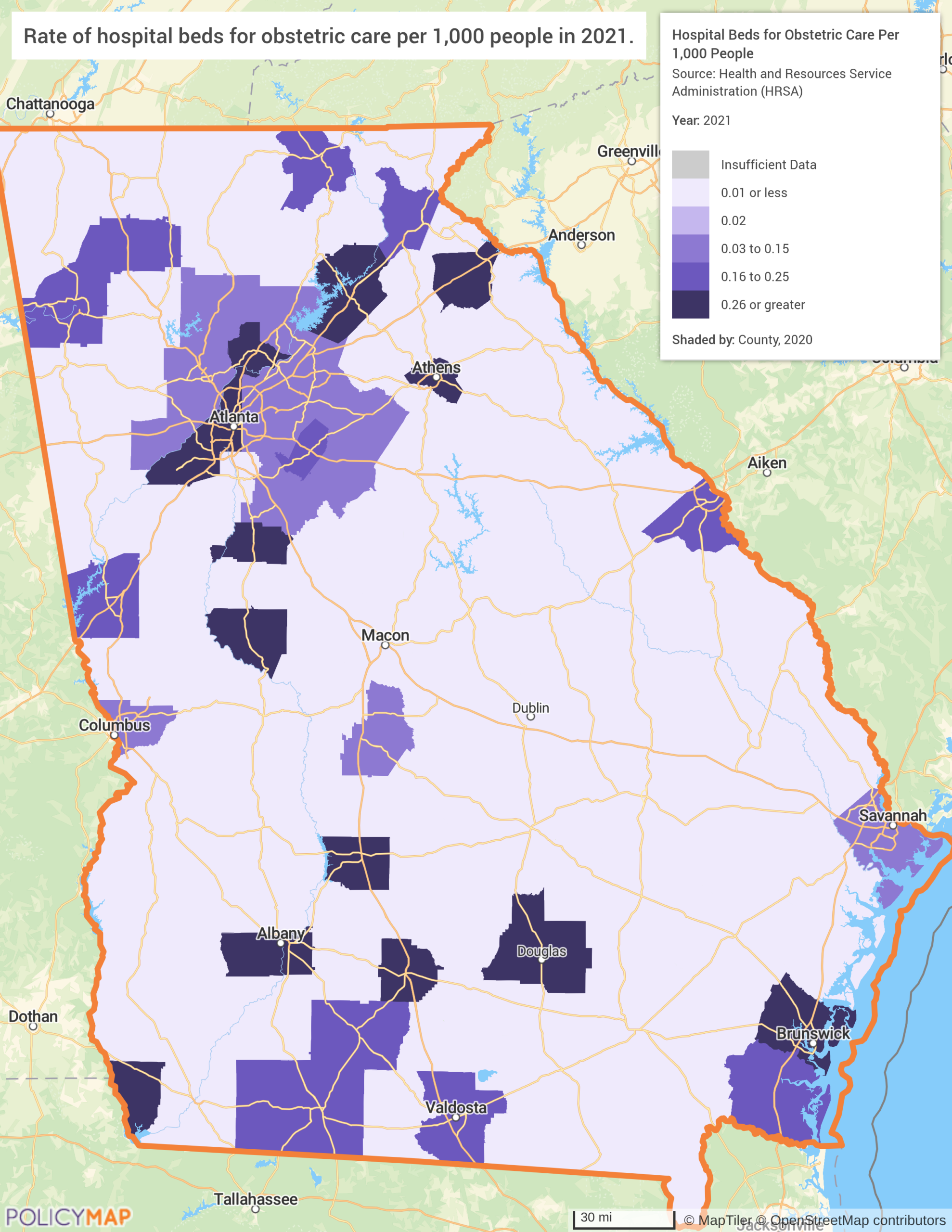
The first map shows the rate of hospital beds and obstetric care per 1,000 residents across Georgia’s counties. The white space is the story; vast stretches of southern and central Georgia register at effectively zero, counties so rural and so devoid of delivery capacity that the data has nothing to show. The dark clusters are Atlanta, Macon, Albany, Columbus, and Savannah. Everything in between, which is most of Georgia geographically, is a void.
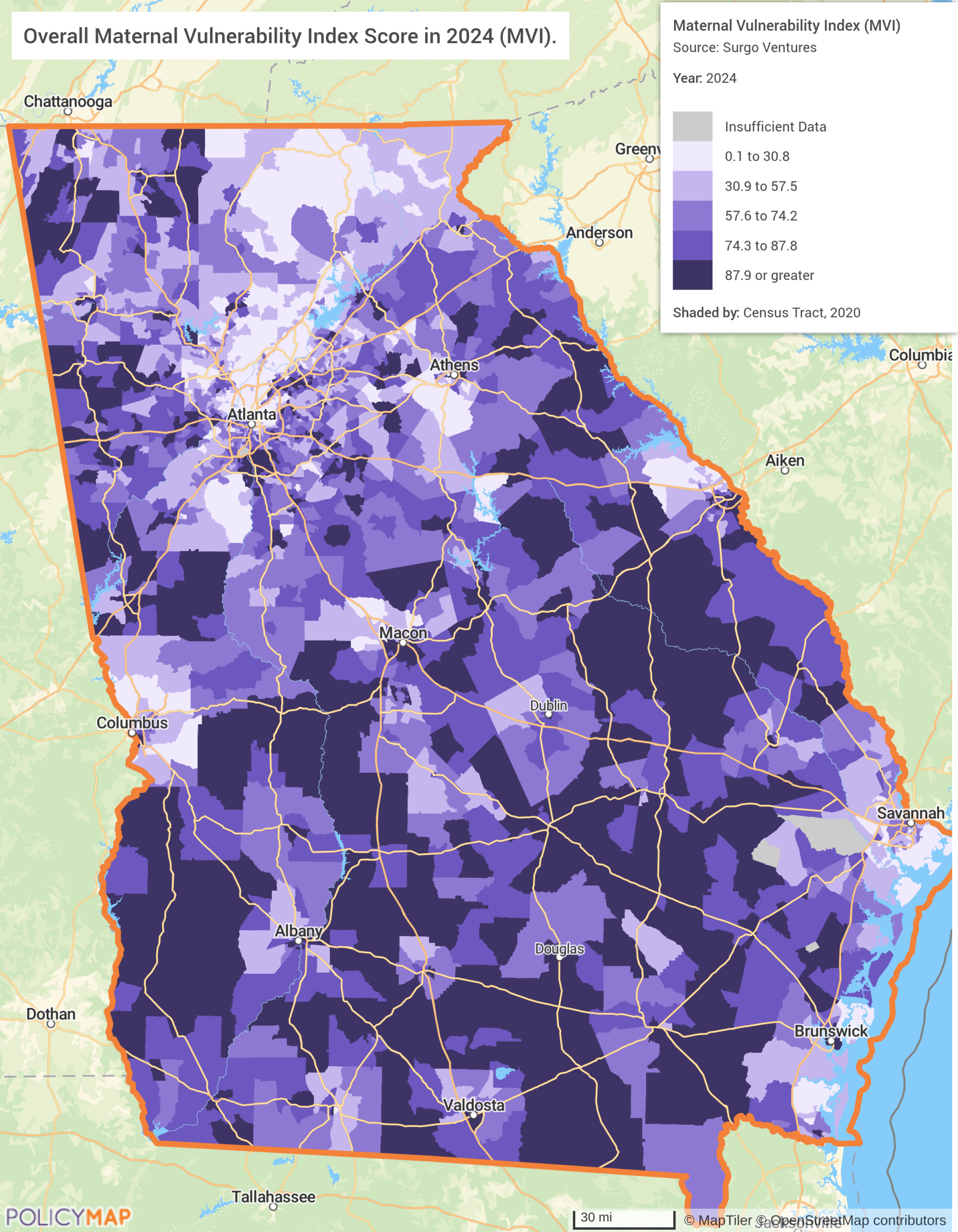
The second map layers the Maternal Vulnerability Index (MVI), a composite score developed by Surgo Ventures that ranks geographies on overall vulnerability to poor pregnancy outcomes across six dimensions: reproductive healthcare access, physical health, mental health and substance use, general healthcare access, socioeconomic determinants, and physical environment. Scored on a scale of 0 to 100 (where 100 represents the highest vulnerability), the MVI captures not just whether care exists, but whether the conditions for a safe pregnancy do. The darkest areas on the map, those with the highest MVI scores, are almost exactly the same geography as the counties with no obstetric capacity on Map 1. The places with no beds are the places where women are most at risk, least insured, and least able to travel for care elsewhere.
Georgia’s situation is severe, but it is not unique. Mississippi has one of the highest maternal mortality rates in the nation and is building a Coordinated Regional Integrated Systems initiative to stabilize rural care delivery. Tennessee has set an explicit goal of eliminating all maternity care deserts in the state by the end of the RHTP funding window. Virginia is deploying mobile prenatal and postpartum care units with a specific focus on mothers with substance use disorders, working to prevent further labor and delivery unit closures. Nebraska, despite its largely agricultural profile, ranks 5th nationally for maternity deserts.
Chronic Disease Management: Arkansas and the Compounding Crisis
Arkansas has the third-highest rate of heart disease mortality in the nation and the highest rate of rural hospital closures, 79% of its rural hospitals are operating at a loss on patient services. These two facts are not unrelated. When providers leave and hospitals close, patients lose access to the preventive care and disease management that keeps chronic conditions from becoming acute crises. Emergency departments absorb the overflow. Costs rise. Outcomes worsen.
Arkansas’s RHTP application responds with the HEART initiative, a six-pronged program spanning all 63 of the state’s counties. It addresses chronic disease and behavioral health together through investments in local food access, recreation infrastructure, child mental health, and telehealth expansion, with a goal of 12,500 residents engaged in health education and screening events through 100 community partners.
The data challenge here is not just mapping where chronic disease rates are high. It is layering that burden against where Medicaid coverage losses are projected to be sharpest. CBO estimates that the OBBBA’s Medicaid provisions will result in roughly 7.5 million people losing coverage by 2034, and rural, Medicaid-dependent communities in states like Arkansas will absorb a disproportionate share of that impact. The communities with the highest disease burden are often the same ones most dependent on the coverage being cut to manage it.
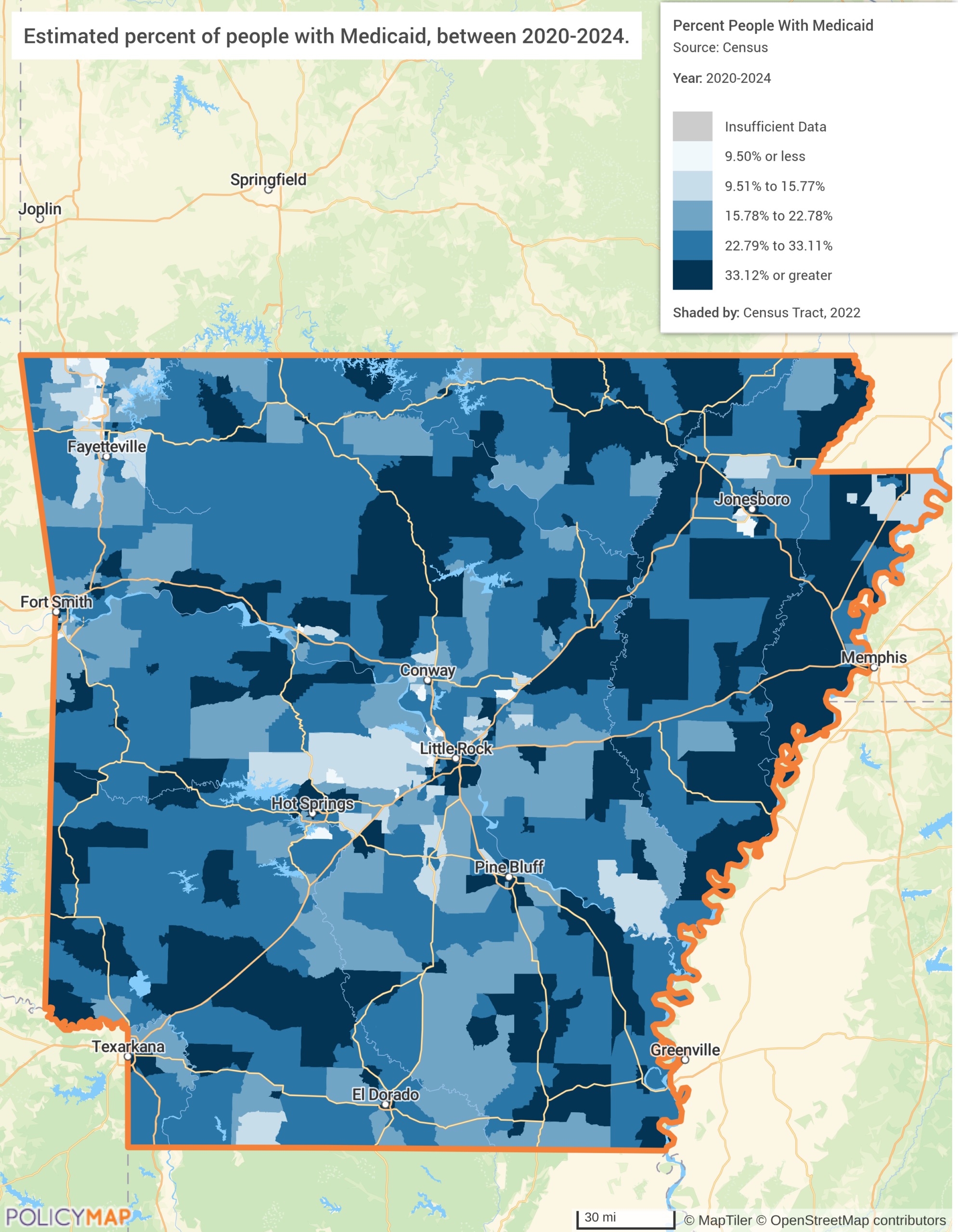
The first map shows Medicaid enrollment rates across Arkansas census tracts. The eastern Delta counties push above 33% Medicaid enrollment. Little Rock and Fayetteville lighten up noticeably; the rural periphery does not. This is the coverage baseline: the communities most exposed to the bill’s Medicaid cuts, and the ones with the least ability to absorb them.
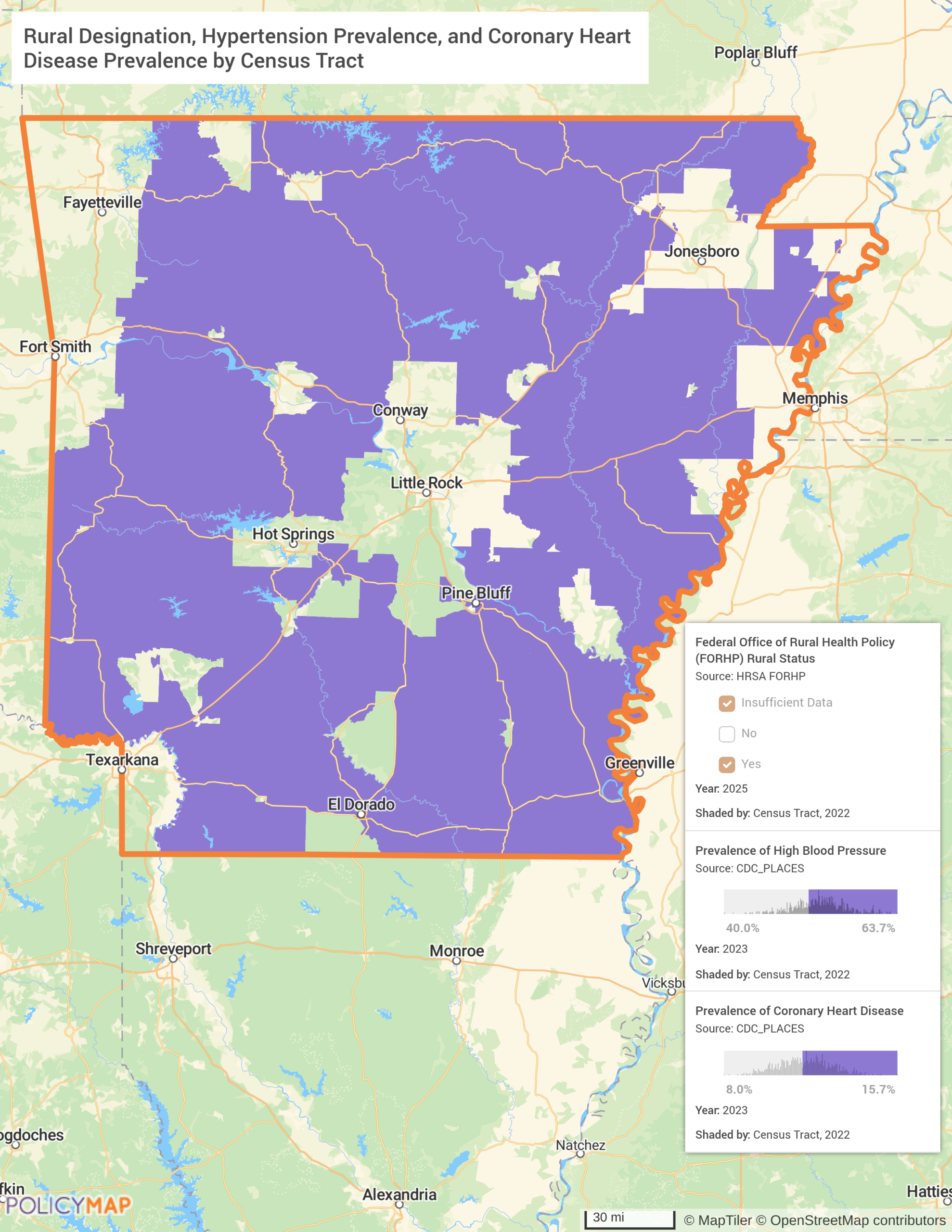
The second map shows why that exposure matters so acutely. Using PolicyMap’s multilayer mapping tool with AND logic (tracts must simultaneously meet all three conditions to appear), nearly the entire state fills in. Rural-designated tracts across Arkansas also carry high blood pressure prevalence rates between 40% and 63.7% and coronary heart disease prevalence between 8% and 15.7%. The exceptions are telling: Little Rock, the Fayetteville corridor, and a handful of scattered urban tracts stay white. Everything else is purple. The cardiovascular burden in Arkansas is not a regional story. It is a statewide one, and it is almost exclusively rural. When those two maps are read together, the policy tension becomes impossible to ignore: the sickest, most rural communities are the most Medicaid-dependent, and those are precisely the communities the bill’s cuts will hit hardest while the RHTP is supposed to help.
Other states are grappling with the same compounding dynamic. Kentucky’s Rural Community Hubs for Chronic Care Innovation target Appalachian counties where diabetes rates are among the highest in the country. Alaska, where 75% of adults carry a chronic disease burden, has made prevention the explicit centerpiece of its transformation plan. Wyoming is building shared-savings chronic disease management programs focused on metabolic and cardiovascular outcomes, using remote patient monitoring to bridge its vast frontier geography.
Workforce Development: Delaware and Building the Pipeline
Delaware ranks last in the nation for meeting primary care needs. Not near the bottom – last. The state’s RHTP response is straightforward in the most literal sense: if you do not have enough doctors, you build a pipeline to train more. Delaware is using its RHTP allocation to fund the state’s first four-year medical school, paired with financial incentives to keep graduates practicing in-state and rural clinical rotations designed to build ties to underserved communities before providers ever finish training.
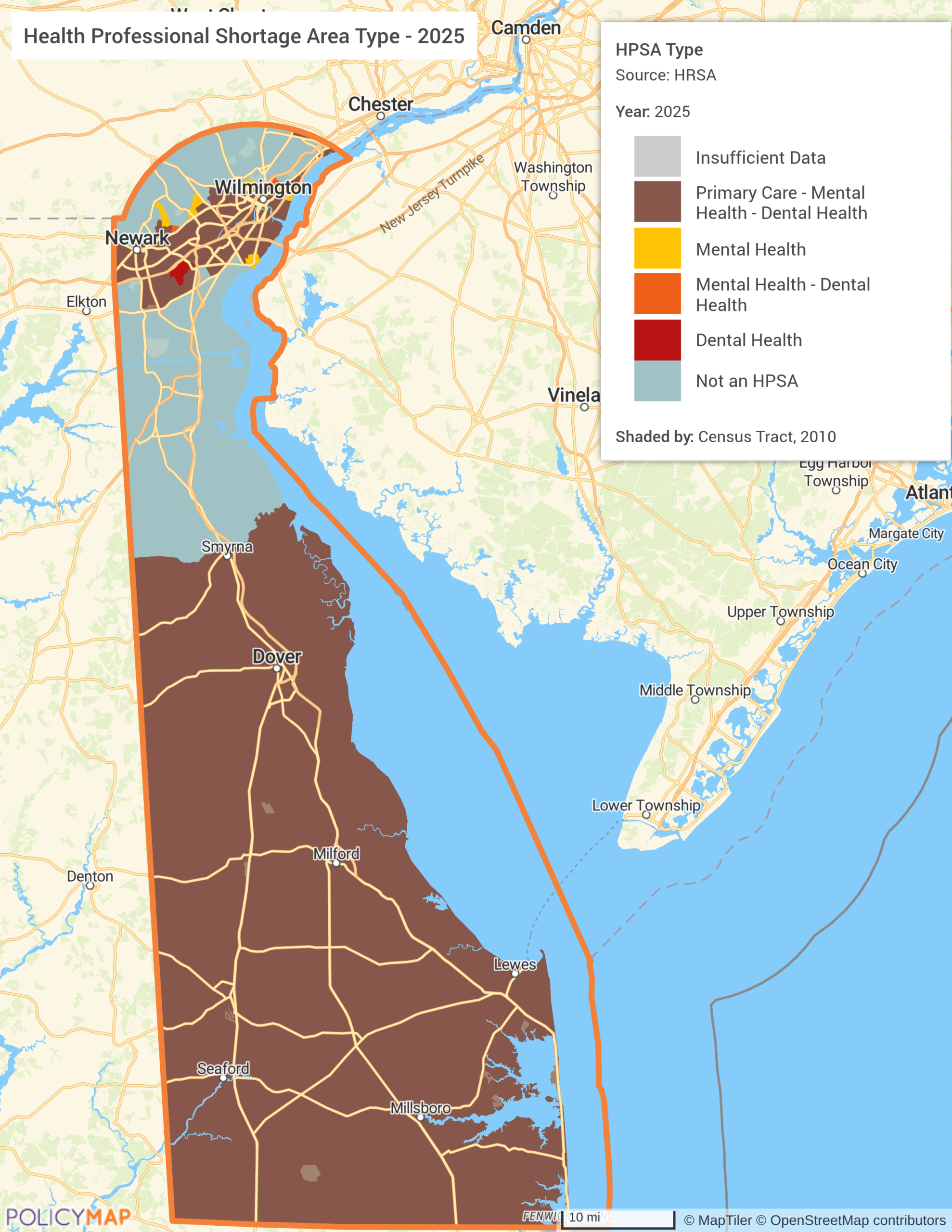
The first map shows Health Professional Shortage Area designations across Delaware by type. The southern two-thirds of the state (Kent and Sussex counties) are designated as shortage areas across primary care, mental health, and dental health simultaneously. Only the Wilmington and Newark corridor in the north escapes the triple designation, and even that urban core carries mental health and dental shortage pockets. The designations confirm the geography of the crisis, but they don’t explain why it persists. For that, you have to look at who is available to fill it.
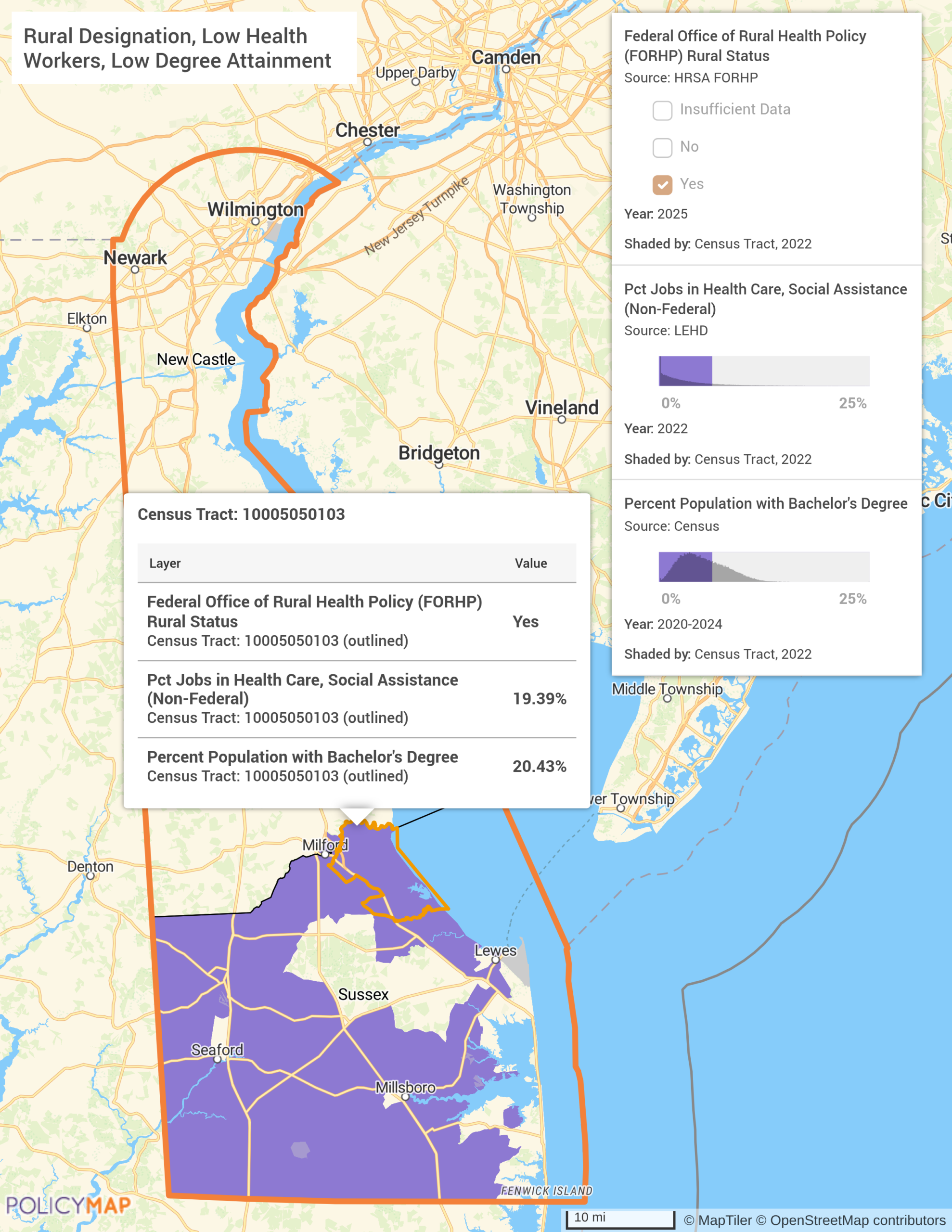
The second map makes the structural argument in a single view. Using PolicyMap’s multilayer tool with AND logic (meaning only tracts that simultaneously meet all three conditions are shown), Sussex County emerges as the state’s most acute convergence point. Its tracts register as HRSA-designated rural, carry low concentrations of health care and social assistance jobs, and have bachelor’s degree attainment rates at the low end of the statewide range. These are not overlapping problems. They are the same problem: a county where the workforce doesn’t exist, the educational pipeline to build one locally is thin, and the federal government has already confirmed the shortage is severe enough to warrant designation. Kent and New Castle counties do not appear. The challenge is concentrated, and it is in Sussex. That is exactly where Delaware’s new medical school, with its rural clinical rotations and in-state retention incentives, needs to reach.
Delaware’s challenge is acute, but its solution, invest in the pipeline before the shortage compounds further, is one that other states are pursuing in different forms. California is building a statewide workforce mapping initiative to track demand trends and pinpoint capacity gaps in real time, ensuring training investments follow need rather than convention. North Dakota is starting even earlier, with “Scrubs Camp” immersion programs for grades 5 through 12 designed to build health career interest in rural communities long before a medical school application is ever filed. Nevada is backing pipeline-building with $80 million in provider incentives to make rural practice a viable destination for graduates once they finish training. The through-line across all of it is the same logic Delaware is betting on: you cannot recruit your way out of a structural shortage. You have to grow out of it.
What $50 Billion Requires
Each of the four focus areas examined here, behavioral health, maternal health, chronic disease management, and workforce development, demands the same foundational capability before a state can move from plan to action: a clear, geographic picture of where need is greatest and where dollars will generate the most impact. The states profiled in this piece are not outliers. They are illustrations of a challenge playing out in every region of the country, in communities that share the same structural disadvantages and face the same impossible math: too little coverage, too few providers, too much disease burden, and now a five-year funding window to do something about it.
That imperative is not just strategic; it is built into the program itself. States must report annually to CMS on measurable outcomes across their chosen investment areas. That reporting requires baseline data. The states that invest in understanding their starting point will be better positioned to demonstrate progress, justify continued investment, and make the case to CMS that their plans are working. The states that don’t will be flying blind into a reporting cycle that begins in 2026 and runs through 2030, with funding renewals dependent on the results.
The geographic patterns visible in these four states repeat across the country. The Delta region’s cardiovascular burden does not stop at the Arkansas border. Obstetric deserts extend well beyond Georgia’s county lines. Behavioral health infrastructure gaps in Wisconsin’s rural north mirror conditions in dozens of other agricultural states. Workforce shortages as acute as Delaware’s exist in states that haven’t yet committed to building a medical school to address them. The data exists to find every one of these convergence points, and to make the case for targeted investment before the window closes.
PolicyMap’s data, including HPSA designations, chronic disease prevalence, mental health and SUD access, maternal health indicators, Medicaid enrollment, rural census tract designations, and more, provides exactly the geographic baseline states, health systems, nonprofits, and community development organizations need to plan, target, and evaluate rural health investments. Whether the goal is identifying where a mobile care unit will reach the most underserved patients, determining which counties face the sharpest Medicaid coverage cliff, or building the evidentiary case for a workforce pipeline investment, the analysis starts with knowing where you are.
Request More Information
$50 billion is on the table, and the clock is running. The communities that can make a data-backed case for their share will be the ones best positioned to use it. Contact PolicyMap to learn how our data and platform can support your rural health planning, grant strategy, or CMS reporting needs.